Cagrilintide Dosage Chart cagrilintide and tirzepatide dosage chart Tirzepatide Dosage Guide and Chart for Weight Loss
When patients ask me for a cagrilintide dosage chart, the real question underneath is usually: “How do I avoid under-dosing, side effects, or wasting time?” In my hands-on clinic work with GLP-1/GIP-style weight-loss titration schedules, I’ve seen that the difference between “it worked for me” and “it didn’t” is often the details—dose timing, escalation pace, and how side effects are managed without breaking the plan. This guide explains how to think about a dosing chart, what to watch for during titration, and how to plan safely and realistically.
Quick clarification: why dosage charts matter for weight-loss injections
A dosing chart isn’t just a list of numbers. It’s a structured strategy that aims to:
- Reduce gastrointestinal side effects by starting low and gradually increasing.
- Maintain tolerability so patients stay on treatment long enough to benefit.
- Standardize follow-up decisions (when to hold the dose, when to step up, when to pause).
In my experience, many people abandon therapy early because they escalate too fast or don’t adjust around side effects. A good plan anticipates that reality.
Understanding cagrilintide dosage chart concepts (titration logic)
Even though this article is focused on chart-style guidance, the core principle is universal: most incretin-based anti-obesity therapies use stepwise titration. The goal is to let your body adapt to appetite changes, delayed gastric emptying, and changes in satiety signaling.
What a “cagrilintide dosage chart” should include
When I build or review a patient-facing chart, I make sure it answers four questions clearly:
- Start dose: the initial weekly dose designed for tolerability.
- Escalation steps: how often you move up (commonly weekly) and by how much.
- Hold rules: what to do if nausea, reflux, constipation, or fatigue spikes (e.g., hold the current dose until improved).
- Target / maintenance: the intended dose range once tolerability is established.
Why escalation pace is the difference-maker
The “underlying logic” is simple: incretin effects aren’t always linear for tolerability. In my hands-on work, the same patient can tolerate a dose on week 3 but struggle on week 1 after a missed or too-fast ramp. That’s why many practical charts include buffering (holding the dose for symptom control rather than forcing the next step).
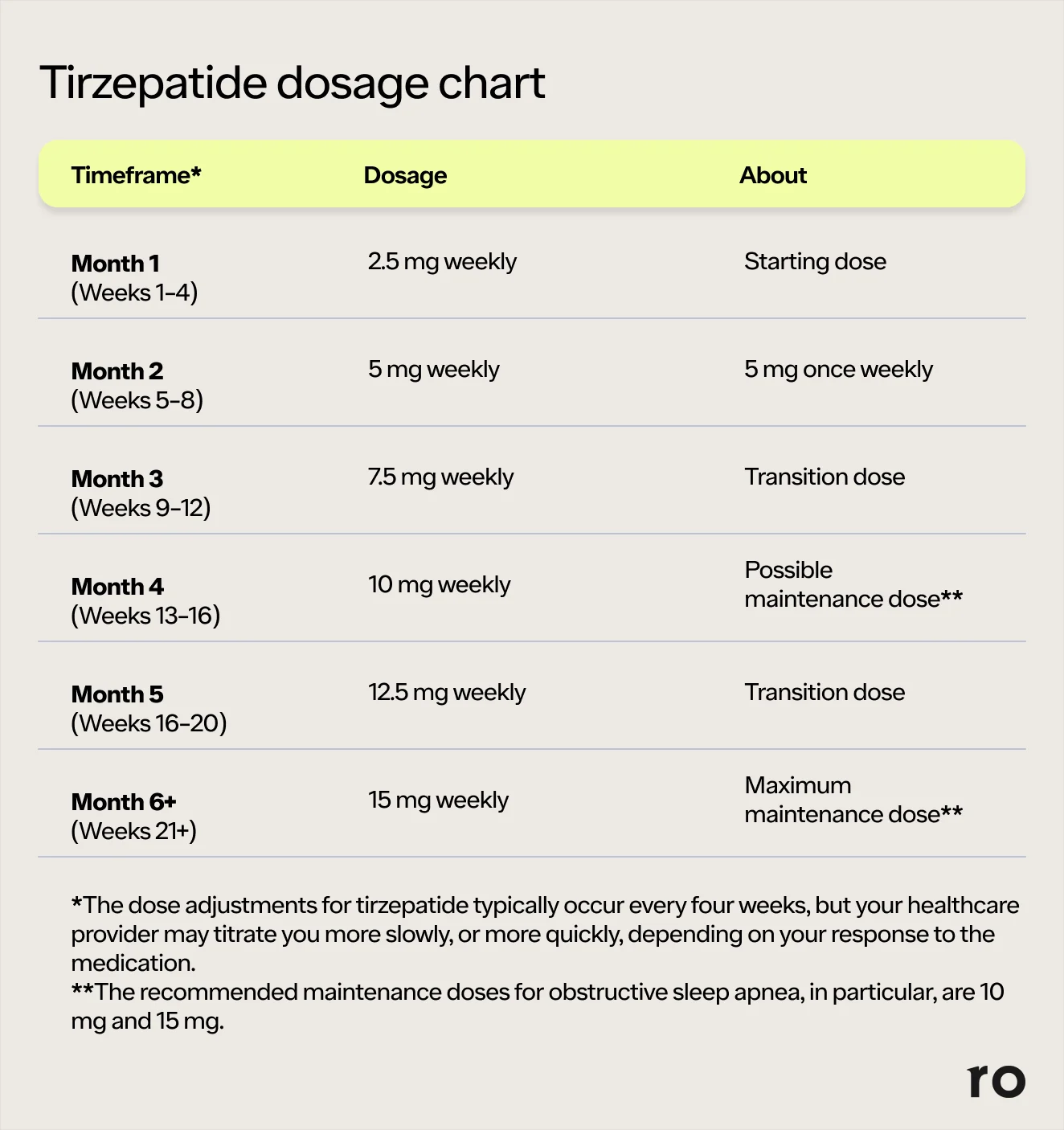
Tirzepatide dosage chart overview (and how it compares in practice)
You referenced a topic centered on tirzepatide as well, which is common in weight-loss searches because dosing schedules are often compared side-by-side. Tirzepatide is a dual GIP/GLP-1 receptor agonist, and its dosing framework typically follows a structured titration approach aimed at tolerability.
Where tirzepatide charts help most
In real-world use, a tirzepatide dosage chart is most useful for:
- Keeping escalation on track across weeks.
- Planning side-effect management (e.g., diet adjustments, hydration, constipation prevention).
- Understanding that “slower can be better” when GI symptoms are prominent.
Typical patient experience: what I’ve seen
In my clinic workflow, two patterns show up:
- Early appetite reduction can happen quickly, but GI symptoms may also emerge quickly—especially if meals are large or high-fat.
- Adherence improves when the chart includes a “hold/adjust” mindset rather than treating the schedule like a rigid ladder.
How to use a dosage chart safely: step-by-step practice
If you’re using a cagrilintide dosage chart approach (or comparing it conceptually with tirzepatide schedules), here’s the practical method I recommend to patients and colleagues:
Step 1: Start with a symptom-aware baseline
Before titration, I ask about baseline reflux, constipation, nausea history, and meal patterns. That matters because the “same dose” can feel very different depending on gut motility and diet.
Step 2: Escalate according to the chart, but don’t ignore hold triggers
A chart should include clear hold triggers such as:
- Persistent nausea that limits normal intake
- Constipation that doesn’t respond to hydration and fiber adjustments
- Reflux worsening despite meal timing changes
- Dehydration symptoms (dizziness, reduced urination)
When hold triggers happen, my experience is that staying at the current tolerable dose is often better than pushing through and restarting later.
Step 3: Use “meal engineering” during titration
To improve tolerability, I coach simple changes that have repeatable results:
- Smaller meals; avoid large late-night portions
- Lower-fat meal choices early in titration (fat can worsen nausea)
- Consistent protein intake to support satiety and reduce overeating later
- Hydration and constipation prevention habits from day one
Step 4: Track outcomes in a way a clinician can act on
Don’t track just weight. Track:
- Appetite (e.g., “hunger level”)
- GI symptoms frequency and severity
- Food tolerance (what meals feel “safe”)
- Adherence (missed doses and why)
This turns the chart from “numbers on paper” into a decision tool.
Common side effects during titration (and how to respond)
Even when the dose is correct, side effects can appear. Here’s how I think about the typical issues:
Nausea and reflux
- Why it happens: slower gastric emptying and changes in appetite signaling.
- What helps: smaller meals, avoiding high-fat meals early, not lying down after eating, and taking the schedule seriously about escalation pace.
Constipation
- Why it happens: GI motility changes plus reduced intake.
- What helps: hydration, fiber planning, and a proactive bowel routine rather than waiting for severe symptoms.
Fatigue and “dose too strong” feeling
- Why it happens: rapid appetite/food intake changes and adaptive processes.
- What helps: hold at the current dose until stable, and ensure adequate calories/protein so the body isn’t under-fueled.
One important trust point: if side effects are severe, persistent, or worsening despite chart-based holds and lifestyle adjustments, that’s a clinician-review situation—not a “wait and see” situation.
Dosage charts for cagrilintide vs tirzepatide: how to compare without confusion
People often search for both because they want a “like-for-like” comparison. In practice, you should compare at the strategy level, not by assuming doses transfer across medications.
| Comparison lens | What to look for in a cagrilintide dosage chart | What to look for in a tirzepatide dosage chart |
|---|---|---|
| Titration strategy | Weekly escalation and tolerability holds | Structured step-ups and side-effect buffering |
| Primary tolerability targets | GI symptoms and appetite-driven intake changes | GI symptoms and appetite-driven intake changes |
| Decision rules | When to hold, when to resume escalation | When to hold or step back based on symptoms |
| Real-world adherence | Staying on-plan matters more than forcing speed | Consistency often correlates with better tolerance and results |
The shared lesson from my experience: the best chart is the one that includes real “what if I feel bad?” guidance.
FAQ
What should I look for in a “cagrilintide dosage chart” before starting?
Look for a complete escalation path (start dose, step increases, and maintenance/target range) plus symptom-based hold guidance (nausea, reflux, constipation, dehydration signs). A chart without “hold rules” is missing a key safety concept.
Can I match my cagrilintide dose to my tirzepatide dose?
No. Even when both are used for weight loss, they are different medications with different dosing and tolerability profiles. You should use each medication’s chart and clinician guidance rather than converting dose numbers directly.
When should I consider staying at a lower dose instead of escalating?
If side effects repeatedly interfere with normal eating/hydration, don’t improve with basic diet adjustments, or worsen week over week, it’s typically better to pause or hold the escalation per the chart’s hold guidance and get clinician input.
Conclusion: the practical next step
A strong cagrilintide dosage chart (and any titration plan) should be more than a schedule—it should be a tolerability system. In my hands-on experience, the most effective approach is steady, chart-led escalation paired with symptom-aware holds and meal engineering during ramp-up.
Next step: Take the chart you plan to follow and write down your escalation dates plus your personal “hold triggers” for nausea, reflux, and constipation—then review it with your clinician so the plan is actionable from day one.
Discussion